
Others like the case for hope Features >>
The Case For Christ
The Case For The Resurrection
The Case For The Resurrection Of Jesus
The Spirit Of The Gospel
He Came To Set The Captives Free
The Leadership Secrets Of Billy Graham
The Reason For God: Belief In An Age Of Scepticism
-160.webp)
The Cross And The Switchblade: A True Story
-160.webp)
Evidence For The Resurrection (What It Means For Your Relationship With God)
-160.webp)
Caring For Creation (The Evangelicals Guide To Climate Change And A Healthy Environment)
About the Book
"The Case for Hope" by Lee Strobel explores the power of hope in the face of life's challenges and hardships. Strobel shares personal stories and insights from experts to make a compelling argument for the importance of hope in navigating difficult circumstances and finding purpose and meaning in life. The book encourages readers to embrace hope and to believe in a brighter future, no matter what they may be facing.
Gladys Aylward
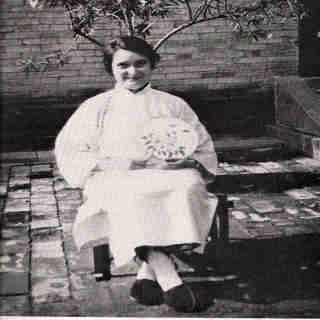 Gladys Aylward was born in London in 1904 (or a few years earlier). She worked for several years as a parlormaid, and then attended a revival meeting at which the preacher spoke of dedicating one's life to the service of God. Gladys responded to the message, and soon after became convinced that she was called to preach the Gospel in China. At the age of 26, she became a probationer at the China Inland Mission Center in London, but was failed to pass the examinations. She worked at other jobs and saved her money. Then she heard of a 73-year-old missionary, Mrs. Jeannie Lawson, who was looking for a younger woman to carry on her work. Gladys wrote to Mrs. Lawson and was accepted if she could get to China. She did not have enough money for the ship fare, but did have enough for the train fare, and so in October of 1930 she set out from London with her passport, her Bible, her tickets, and two pounds ninepence, to travel to China by the Trans-Siberian Railway, despite the fact that China and the Soviet Union were engaged in an undeclared war. She arrived in Vladivostok and sailed from there to Japan and from Japan to Tientsin, and thence by train, then bus, then mule, to the inland city of Yangchen, in the mountainous province of Shansi, a little south of Peking (Beijing). Most of the residents had seen no Europeans other than Mrs. Lawson and now Miss Aylward. They distrusted them as foreigners, and were not disposed to listen to them.
Yangchen was an overnight stop for mule caravans that carried coal, raw cotton, pots, and iron goods on six-week or three-month journeys. It occurred to the two women that their most effective way of preaching would be to set up an inn. The building in which they lived had once been an inn, and with a bit of repair work could be used as one again. They laid in a supply of food for mules and men, and when next a caravan came past, Gladys dashed out, grabbed the rein of the lead mule, and turned it into their courtyard. It went willingly, knowing by experience that turning into a courtyard meant food and water and rest for the night. The other mules followed, and the muleteers had no choice. They were given good food and warm beds at the standard price, and their mules were well cared for, and there was free entertainment in the evening--the inkeepers told stories about a man named Jesus. After the first few weeks, Gladys did not need to kidnap customers -- they turned in at the inn by preference. Some became Christians, and many of them (both Christians and non-Christians) remembered the stories, and retold them more or less accurately to other muleteers at other stops along the caravan trails. Gladys practiced her Chinese for hours each day, and was becoming fluent and comfortable with it. Then Mrs. Lawson suffered a severe fall, and died a few days later. Gladys Aylward was left to run the mission alone, with the aid of one Chinese Christian, Yang, the cook.
A few weeks after the death of Mrs. Lawson, Miss Aylward met the Mandarin of Yangchen. He arrived in a sedan chair, with an impressive escort, and told her that the government had decreed an end to the practice of footbinding. (Note: Among the upper and middle classes, it had for centuries been the custom that a woman's foot should be wrapped tightly in bandages from infancy, to prevent it from growing. Thus grown women had extremely tiny feet, on which they could walk only with slow, tottering steps, which were thought to be extremely graceful.) The government needed a foot-inspector, a woman (so that she could invade the women's quarters without scandal), with her own feet unbound (so that she could travel), who would patrol the district enforcing the decree. It was soon clear to them both that Gladys was the only possible candidate for the job, and she accepted, realizing that it would give her undreamed-of opportunities to spread the Gospel.
During her second year in Yangchen, Gladys was summoned by the Mandarin. A riot had broken out in the men's prison. She arrived and found that the convicts were rampaging in the prison courtyard, and several of them had been killed. The soldiers were afraid to intervene. The warden of the prison said to Gladys, "Go into the yard and stop the rioting." She said, "How can I do that?" The warden said, "You have been preaching that those who trust in Christ have nothing to fear." She walked into the courtyard and shouted: "Quiet! I cannot hear when everyone is shouting at once. Choose one or two spokesmen, and let me talk with them." The men quieted down and chose a spokesman. Gladys talked with him, and then came out and told the warden: "You have these men cooped up in crowded conditions with absolutely nothing to do. No wonder they are so edgy that a small dispute sets off a riot. You must give them work. Also, I am told that you do not supply food for them, so that they have only what their relatives send them. No wonder they fight over food. We will set up looms so that they can weave cloth and earn enough money to buy their own food." This was done. There was no money for sweeping reforms, but a few friends of the warden donated old looms, and a grindstone so that the men could work grinding grain. The people began to call Gladys Aylward "Ai-weh-deh," which means "Virtuous One." It was her name from then on.
Soon after, she saw a woman begging by the road, accompanied by a child covered with sores and obviously suffering severe malnutrition. She satisfied herself that the woman was not the child's mother, but had kidnapped the child and was using it as an aid to her begging. She bought the child for ninepence--a girl about five years old. A year later, "Ninepence" came in with an abandoned boy in tow, saying, "I will eat less, so that he can have something." Thus Ai-weh-deh acquired a second orphan, "Less." And so her family began to grow.... She was a regular and welcome visitor at the palace of the Mandarin, who found her religion ridiculous, but her conversation stimulating. In 1936, she officially became a Chinese citizen. She lived frugally and dressed like the people around her (as did the missionaries who arrived a few years after in in the neighboring town of Tsechow, David and Jean Davis and their young son Murray, of Wales), and this was a major factor in making her preaching effective.
Then the war came. In the spring of 1938, Japanese planes bombed the city of Yangcheng, killing many and causing the survivors to flee into the mountains. Five days later, the Japanese Army occupied Yangcheng, then left, then came again, then left. The Mandarin gathered the survivors and told them to retreat into the mountains for the duration. He also announced that he was impressed by the life of Ai-weh-deh and wished to make her faith his own. There remained the question of the convicts at the jail. The traditional policy favored beheading them all lest they escape. The Mandarin asked Ai-weh-deh for advice, and a plan was made for relatives and friends of the convicts to post a bond guaranteeing their good behavior. Every man was eventually released on bond. As the war continued Gladys often found herself behind Japanese lines, and often passed on information, when she had it, to the armies of China, her adopted country. She met and became friends with "General Ley," a Roman Catholic priest from Europe who had teken up arms when the Japanese invaded, and now headed a guerilla force. Finally he sent her a message. The Japanese are coming in full force. We are retreating. Come with us." Angry, she scrawled a Chinese note, Chi Tao Tu Pu Twai, "Christians never retreat!" He sent back a copy of a Japanese handbill offering $100 each for the capture, dead or alive, of (1) the Mandarin, (2) a prominent merchant, and (3) Ai-weh-deh. She determined to flee to the government orphanage at Sian, bringing with her the children she had accumulated, about 100 in number. (An additional 100 had gone ahead earlier with a colleague.) With the children in tow, she walked for twelve days. Some nights they found shelter with friendly hosts. Some nights they spent unprotected on the mountainsides. On the twelfth day, they arrived at the Yellow River, with no way to cross it. All boat traffic had stopped, and all civilian boats had been seized to keep them out of the hands of the Japanese. The children wanted to know, "Why don't we cross?" She said, "There are no boats." They said, "God can do anything. Ask Him to get us across." They all knelt and prayed. Then they sang. A Chinese officer with a patrol heard the singing and rode up. He heard their story and said, "I think I can get you a boat." They crossed, and after a few more difficulties Ai-weh-deh delivered her charges into competent hands at Sian, and then promptly collapsed with typhus fever and sank into delirium for several days.
As her health gradually improved, she started a Christian church in Sian, and worked elsewhere, including a settlement for lepers in Szechuan, near the borders of Tibet. Her health was permanently impaired by injuries received during the war, and in 1947 she returned to England for a badly needed operation. She remained in England, preaching there.
In 1957, Alan Burgess wrote a book about her, The Small Woman. It was condensed in The Reader's Digest, and made into a movie called The Inn of the Sixth Happiness, starring Ingrid Bergman. When Newsweek magazine reviewed the movie, and summarized the plot, a reader, supposing the story to be fiction, wrote in to say, "In order for a movie to be good, the story should be believable!" Miss Gladys Aylward, the Small Woman, Ai-weh-deh, died 3 January 1970.
Gladys Aylward was born in London in 1904 (or a few years earlier). She worked for several years as a parlormaid, and then attended a revival meeting at which the preacher spoke of dedicating one's life to the service of God. Gladys responded to the message, and soon after became convinced that she was called to preach the Gospel in China. At the age of 26, she became a probationer at the China Inland Mission Center in London, but was failed to pass the examinations. She worked at other jobs and saved her money. Then she heard of a 73-year-old missionary, Mrs. Jeannie Lawson, who was looking for a younger woman to carry on her work. Gladys wrote to Mrs. Lawson and was accepted if she could get to China. She did not have enough money for the ship fare, but did have enough for the train fare, and so in October of 1930 she set out from London with her passport, her Bible, her tickets, and two pounds ninepence, to travel to China by the Trans-Siberian Railway, despite the fact that China and the Soviet Union were engaged in an undeclared war. She arrived in Vladivostok and sailed from there to Japan and from Japan to Tientsin, and thence by train, then bus, then mule, to the inland city of Yangchen, in the mountainous province of Shansi, a little south of Peking (Beijing). Most of the residents had seen no Europeans other than Mrs. Lawson and now Miss Aylward. They distrusted them as foreigners, and were not disposed to listen to them.
Yangchen was an overnight stop for mule caravans that carried coal, raw cotton, pots, and iron goods on six-week or three-month journeys. It occurred to the two women that their most effective way of preaching would be to set up an inn. The building in which they lived had once been an inn, and with a bit of repair work could be used as one again. They laid in a supply of food for mules and men, and when next a caravan came past, Gladys dashed out, grabbed the rein of the lead mule, and turned it into their courtyard. It went willingly, knowing by experience that turning into a courtyard meant food and water and rest for the night. The other mules followed, and the muleteers had no choice. They were given good food and warm beds at the standard price, and their mules were well cared for, and there was free entertainment in the evening--the inkeepers told stories about a man named Jesus. After the first few weeks, Gladys did not need to kidnap customers -- they turned in at the inn by preference. Some became Christians, and many of them (both Christians and non-Christians) remembered the stories, and retold them more or less accurately to other muleteers at other stops along the caravan trails. Gladys practiced her Chinese for hours each day, and was becoming fluent and comfortable with it. Then Mrs. Lawson suffered a severe fall, and died a few days later. Gladys Aylward was left to run the mission alone, with the aid of one Chinese Christian, Yang, the cook.
A few weeks after the death of Mrs. Lawson, Miss Aylward met the Mandarin of Yangchen. He arrived in a sedan chair, with an impressive escort, and told her that the government had decreed an end to the practice of footbinding. (Note: Among the upper and middle classes, it had for centuries been the custom that a woman's foot should be wrapped tightly in bandages from infancy, to prevent it from growing. Thus grown women had extremely tiny feet, on which they could walk only with slow, tottering steps, which were thought to be extremely graceful.) The government needed a foot-inspector, a woman (so that she could invade the women's quarters without scandal), with her own feet unbound (so that she could travel), who would patrol the district enforcing the decree. It was soon clear to them both that Gladys was the only possible candidate for the job, and she accepted, realizing that it would give her undreamed-of opportunities to spread the Gospel.
During her second year in Yangchen, Gladys was summoned by the Mandarin. A riot had broken out in the men's prison. She arrived and found that the convicts were rampaging in the prison courtyard, and several of them had been killed. The soldiers were afraid to intervene. The warden of the prison said to Gladys, "Go into the yard and stop the rioting." She said, "How can I do that?" The warden said, "You have been preaching that those who trust in Christ have nothing to fear." She walked into the courtyard and shouted: "Quiet! I cannot hear when everyone is shouting at once. Choose one or two spokesmen, and let me talk with them." The men quieted down and chose a spokesman. Gladys talked with him, and then came out and told the warden: "You have these men cooped up in crowded conditions with absolutely nothing to do. No wonder they are so edgy that a small dispute sets off a riot. You must give them work. Also, I am told that you do not supply food for them, so that they have only what their relatives send them. No wonder they fight over food. We will set up looms so that they can weave cloth and earn enough money to buy their own food." This was done. There was no money for sweeping reforms, but a few friends of the warden donated old looms, and a grindstone so that the men could work grinding grain. The people began to call Gladys Aylward "Ai-weh-deh," which means "Virtuous One." It was her name from then on.
Soon after, she saw a woman begging by the road, accompanied by a child covered with sores and obviously suffering severe malnutrition. She satisfied herself that the woman was not the child's mother, but had kidnapped the child and was using it as an aid to her begging. She bought the child for ninepence--a girl about five years old. A year later, "Ninepence" came in with an abandoned boy in tow, saying, "I will eat less, so that he can have something." Thus Ai-weh-deh acquired a second orphan, "Less." And so her family began to grow.... She was a regular and welcome visitor at the palace of the Mandarin, who found her religion ridiculous, but her conversation stimulating. In 1936, she officially became a Chinese citizen. She lived frugally and dressed like the people around her (as did the missionaries who arrived a few years after in in the neighboring town of Tsechow, David and Jean Davis and their young son Murray, of Wales), and this was a major factor in making her preaching effective.
Then the war came. In the spring of 1938, Japanese planes bombed the city of Yangcheng, killing many and causing the survivors to flee into the mountains. Five days later, the Japanese Army occupied Yangcheng, then left, then came again, then left. The Mandarin gathered the survivors and told them to retreat into the mountains for the duration. He also announced that he was impressed by the life of Ai-weh-deh and wished to make her faith his own. There remained the question of the convicts at the jail. The traditional policy favored beheading them all lest they escape. The Mandarin asked Ai-weh-deh for advice, and a plan was made for relatives and friends of the convicts to post a bond guaranteeing their good behavior. Every man was eventually released on bond. As the war continued Gladys often found herself behind Japanese lines, and often passed on information, when she had it, to the armies of China, her adopted country. She met and became friends with "General Ley," a Roman Catholic priest from Europe who had teken up arms when the Japanese invaded, and now headed a guerilla force. Finally he sent her a message. The Japanese are coming in full force. We are retreating. Come with us." Angry, she scrawled a Chinese note, Chi Tao Tu Pu Twai, "Christians never retreat!" He sent back a copy of a Japanese handbill offering $100 each for the capture, dead or alive, of (1) the Mandarin, (2) a prominent merchant, and (3) Ai-weh-deh. She determined to flee to the government orphanage at Sian, bringing with her the children she had accumulated, about 100 in number. (An additional 100 had gone ahead earlier with a colleague.) With the children in tow, she walked for twelve days. Some nights they found shelter with friendly hosts. Some nights they spent unprotected on the mountainsides. On the twelfth day, they arrived at the Yellow River, with no way to cross it. All boat traffic had stopped, and all civilian boats had been seized to keep them out of the hands of the Japanese. The children wanted to know, "Why don't we cross?" She said, "There are no boats." They said, "God can do anything. Ask Him to get us across." They all knelt and prayed. Then they sang. A Chinese officer with a patrol heard the singing and rode up. He heard their story and said, "I think I can get you a boat." They crossed, and after a few more difficulties Ai-weh-deh delivered her charges into competent hands at Sian, and then promptly collapsed with typhus fever and sank into delirium for several days.
As her health gradually improved, she started a Christian church in Sian, and worked elsewhere, including a settlement for lepers in Szechuan, near the borders of Tibet. Her health was permanently impaired by injuries received during the war, and in 1947 she returned to England for a badly needed operation. She remained in England, preaching there.
In 1957, Alan Burgess wrote a book about her, The Small Woman. It was condensed in The Reader's Digest, and made into a movie called The Inn of the Sixth Happiness, starring Ingrid Bergman. When Newsweek magazine reviewed the movie, and summarized the plot, a reader, supposing the story to be fiction, wrote in to say, "In order for a movie to be good, the story should be believable!" Miss Gladys Aylward, the Small Woman, Ai-weh-deh, died 3 January 1970.
the sluggard in me - four lies that lead to lazy
Come, follow closely, and gaze for a moment upon a rare creature in his native habitat. There he is, drooling upon his pillow an hour before lunchtime, creaking over the bedsprings like a door on its hinges. “How long will you lie there? When will you arise from your sleep?” his mother shouts from the kitchen. Quiet, now: she has roused him. Here he comes, stumbling into his chair, and begins to feed. “What’s wrong with a little sleep, a little slumber?” he mumbles between mouthfuls. A dozen handfuls later, however, he stops, his hand submerged in his cereal like a sunk boat. He breathes heavily, chin against his chest, and begins to snore again. Meet the sluggard (Proverbs 26:14; 6:9–10; 19:24). He is a figure of “tragi-comedy,” Derek Kidner writes ( Proverbs , 39): comedy, because the sluggard’s laziness makes him ludicrous; tragedy, because only sin could so debase a man. The image of God was never meant to yawn through life. Yet those who are paying attention will also see something more in this tragi-comic sloth: themselves. We all have an inner sluggard, counseling us to sleep when we should rise, rest when we should work, eat when we should move. “The wise man,” Kidner goes on to write, knows that the sluggard is no freak, but, as often as not, an ordinary man who has made too many excuses, too many refusals, and too many postponements. It has all been as imperceptible, and as pleasant, as falling asleep. (40) We don’t need to look far, then, to see the sluggard in his native habitat. We only need to hear his “excuses,” “refusals,” and “postponements,” and then listen for their inner echo. ‘I need just a little more.’ A little sleep, a little slumber, a little folding of the hands to rest. (Proverbs 6:10; 24:33) The words sit in the mouth of the sluggard more than once in Proverbs. They are, perhaps, his motto, his favorite response to the wisdom of the diligent. “Early to rest, early to rise . . .” they tell him; “A little sleep, a little slumber . . .” he answers. “An ordinary man becomes a sluggard one small surrender at a time.” Sluggishness often hides beneath that eminently reasonable phrase “just a little more.” What harm could a little do? What’s one more snooze cycle? What’s one more show? What’s one more refreshing of the timeline? Not much, in itself: but much indeed when piled atop ten thousand other littles and one mores . They may seem like “small surrenders” (to use a phrase from Bruce Waltke, Proverbs , 131) — and they are. But an ordinary man becomes a sluggard one small surrender at a time. How do the wise respond? They know that diligent Christians are not a special species of saint. Like the sluggard, the diligent daily face unpleasant tasks. Unlike the sluggard, the diligent speak a different motto: “A little labor, a little energy, a little moving of the hands to work.” Instead of building a stack of small surrenders, they build a stack of small successes — taking little step by little step in the strength that God supplies. Over time, how we handle little is no little matter. Little drudgeries, little tasks, little opportunities: these are the moments when the sluggard gains ground in our souls, or loses it. ‘There’s always tomorrow.’ The sluggard does not plow in the autumn; he will seek at harvest and have nothing. (Proverbs 20:4) Often enough, “just a little more” achieves the sluggard’s purpose. But if, for some reason, his conscience should protest, he has another word at his disposal that rarely fails: tomorrow . Autumn was the season for plowing and planting in ancient Israel, and summer the season for harvest. We don’t know exactly why the sluggard took it easy while his neighbors plowed their fields. Maybe the difficulty of the task daunted him, or maybe, as the King James Version suggests, the season’s chill deterred him: “The sluggard will not plow by reason of the cold .” Either way, he no doubt fell asleep on many autumn nights warmed by the thought, “There’s always tomorrow” — until one day he woke up in winter. When the sluggard finally arrived at his chosen tomorrow , the time for plowing and planting had escaped his grasp. How often have we too discovered that tomorrow is too late? The conversation we should have initiated yesterday proves more awkward today. The essay we should have begun last week overwhelms us this week. The forgiveness we should have sought last month feels harder to seek this month. Autumn has passed, winter has come, and opportunity has slipped through our fingers. The wise learn to take the farmer’s view of life: when the time comes to plow, a farmer pays more attention to the season than to his feelings. And when the time comes to tackle our own difficult tasks, the wise do the same. ‘I would be putting myself at risk.’ There is a lion outside! I shall be killed in the streets! (Proverbs 22:13; see also 26:13) Indulging a bad excuse is a little like feeding a pigeon: give bread to one, and twenty more will soon coo at your feet. Bad excuses breed bad excuses — and even worse excuses over time. And so, when a friend, family member, or boss refuses to entertain the sluggard’s littles and tomorrows , he takes more radical measures: “Haven’t you seen the lion roaming the streets? I’ll die!” Did any sluggard ever attempt such an excuse? Maybe. “Laziness is a great lion-maker,” says Charles Spurgeon. “He who does little dreams much. His imagination could create not only a lion but a whole menagerie of wild beasts” (“One Lion: Two Lions: No Lion at All”). For our own purposes, however, we can consider a tamer version of the sluggard’s beast: “I would be putting myself at risk.” To our inner sluggard, a scratch in the throat is cause for a sick day, a little tiredness is reason to nap instead of mow, and a long day at work is justification for skipping small group. After all, our bodies and minds need the rest, don’t they? Care is required here, of course. Some people really do work their bodies into the dust, forsaking the rest God gives and “eating the bread of anxious toil” (Psalm 127:2). The sluggard, however, is prone to label as “anxious toil” any work that meets with inner resistance. He forgets that overcoming such resistance is part of what makes diligence diligence . God made our bodies to bend and strain, our minds to crank and labor, our souls to strive and press. The lion called “Lazy” will counsel us to avoid the strain, but diligence will slay the lion. ‘What do you know about the pressures I’m under?’ The sluggard is wiser in his own eyes than seven men who can answer sensibly. (Proverbs 26:16) Confront a sluggard in his sluggishness, and you may find that he has a penchant for euphemisms. “He has no idea that he is lazy,” writes Kidner on Proverbs 26:13–16. He is not a shirker but a “realist” (13); not self-indulgent but “below his best in the morning” (14); his inertia is “an objection to being hustled” (15); his mental indolence a fine “sticking to his guns” (16). ( Proverbs , 156) Our own sluggishness, then, often appears in our defenses against the charge. Once, as a single man, I told a mentor, “I need more time to myself.” “You don’t need it,” he responded. Immediately, I raised the drawbridge, manned the ramparts, and launched inward mortars against the attack. What could he, a husband and father of three, possibly know about the pressures I was under? The self-defense is laughable now, but back then, wise in my own eyes, I couldn’t accept that much of what I called “alone time” was better labeled “sluggishness.” The sluggard sees his own work as the hardest work, his own excuses as the best excuses, his own diversions as the most reasonable diversions — no matter what his friends, wife, or pastor may say. But the wise learn to develop a self-distrustful posture. Rather than responding to requests or challenges with an inward Don’t you see my burdens? they remember their proneness to folly, and learn to call the sluggard by his real name. The Christian and the Sluggard Between the Christian and the sluggard, Spurgeon says, “there should be as wide a division as between the poles.” He’s right. “Christian” and “sluggard” go together like “husband” and “playboy,” like “judge” and “thief”: the latter destroys the integrity of the former. “In Christ we find our pattern for work. In Christ we find our power for work. And in Christ the sluggard dies.” And why? Because Christians belong to Jesus Christ, and Jesus Christ was not sluggish. He was no workaholic, of course: he could feast, rest, sleep, and develop deep relationships. But oh did he work. In the Gospels we find not the sluggishness but “the steadfastness of Christ” (2 Thessalonians 3:5): the diligence of one who never entertained “just a little more” or “tomorrow,” but worked while it was day (John 9:4). He plowed in the autumn cold of life, forsaking every excuse not to save us. And he never cried “lion!” though he walked into the den (Psalm 22:21). Therefore, the apostle Paul can say to the sluggish, “Such persons we command and encourage in the Lord Jesus Christ to do their work” (2 Thessalonians 3:12). In Christ we find our pattern for work. In Christ we find our power for work. And in Christ the sluggard dies.